Transsphenoidal Surgery6
Study description
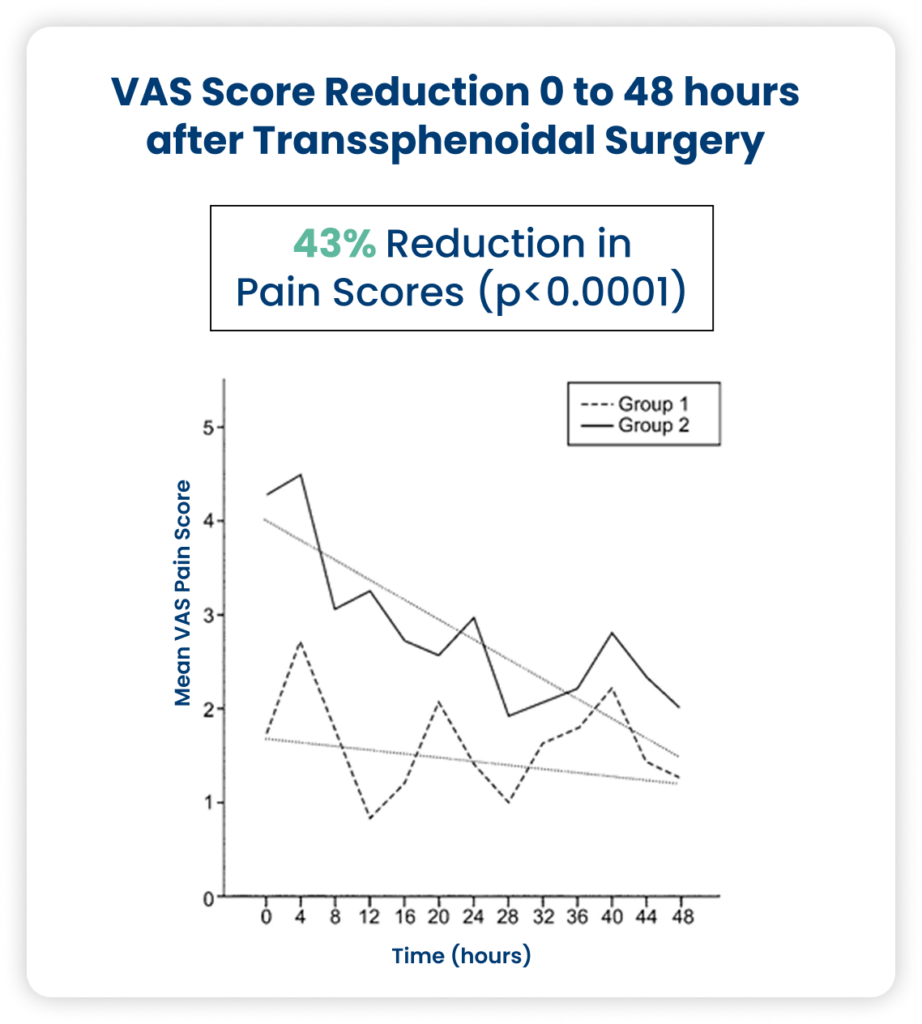
Single-center, randomized, double-blind, placebo-controlled intervention trial in adult patients undergoing transsphenoidal surgery for pituitary adenoma.
Randomized to
- Group 1: scheduled Caldolor IV 800 mg q 8 hr + scheduled oral acetaminophen 1000 mg PO q 6 hr + rescue opioids
OR
- Group 2: IV placebo + scheduled oral acetaminophen + rescue opioids
Primary Outcome: pain scores (VAS, rated 0-10) every 4 hours for 48 hours after surgery.
Secondary Outcome: opioid use in the 1st 48 hours after surgery, estimated by oral morphine equivalents.
N = 62
- Group 1 = 28
- Group 2 = 34
Elective Orthopedic2
Study description
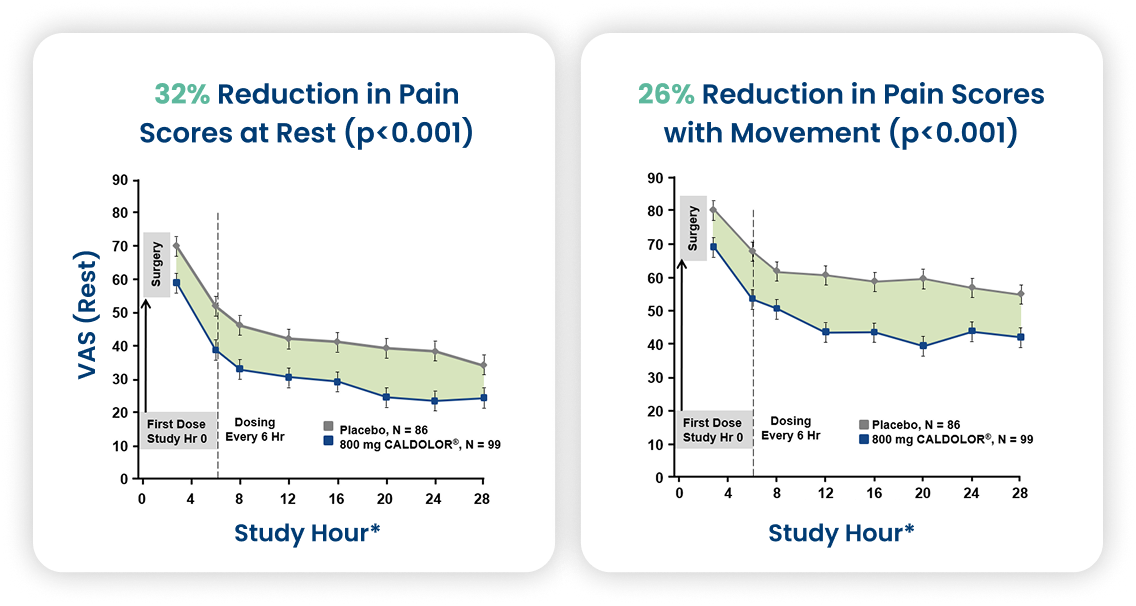
Multi-center, randomized, double-blind, placebo-controlled in patients undergoing elective orthopedic surgery.
Randomized 1:1 Caldolor 800 mg or placebo
- Administered pre-op and every 6 hours
- Morphine PCA for breakthrough pain
Primary Outcome: Self-reported pain assessment scores at rest and with movement at hours 6-28 post-op
Secondary Outcomes: Morphine requirement at hour 28 post-op
N = 185
- Caldolor = 99
- Placebo = 86
Arthroscopic Knee16
Study description
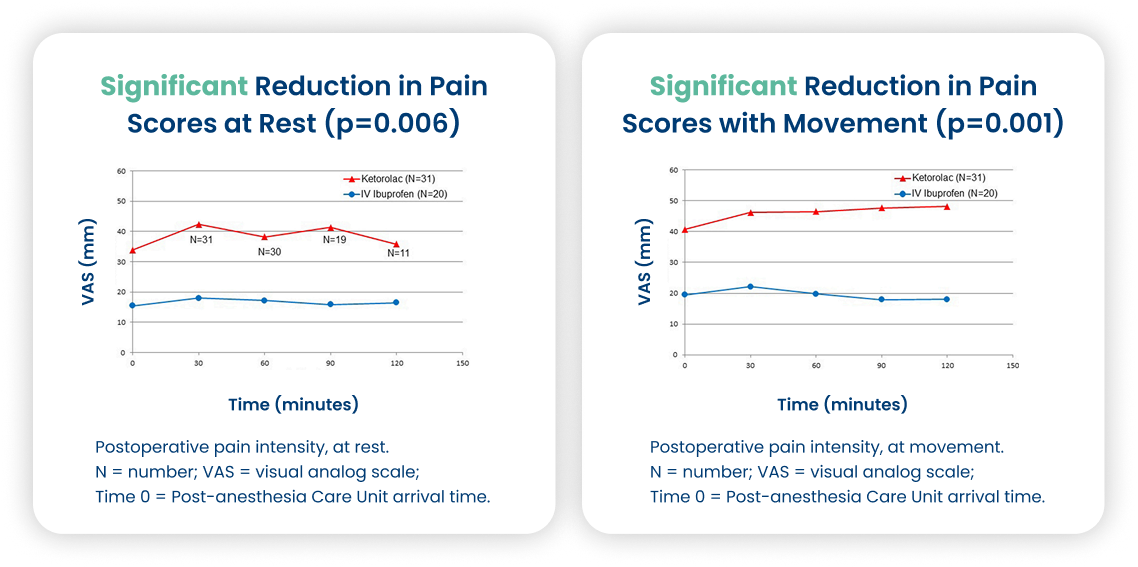
Single-center, randomized, double-blind, parallel, active comparator in patients undergoing arthroscopic knee surgery.
Randomized:
- Caldolor 800 mg IV x 2 administered pre-op and then 4 hours later
- IV Ketorolac 30 mg at end of surgery
- IV Hydromorphine PRN in PACU for breakthrough
Primary Outcome: Self-assessment pain scores at rest and movement
- Every 30 min until PACU discharge and then at 24 hours
Secondary Outcome: Breakthrough pain medication required at 24 hours post-op, adverse events, satisfaction questionnaire.
N = 53 (2 excluded later due to failing to meet criteria)
- Caldolor 800mg = 20
- Ketorolac = 31
Oral Surgery: Third Molar Removal18
Outcomes:
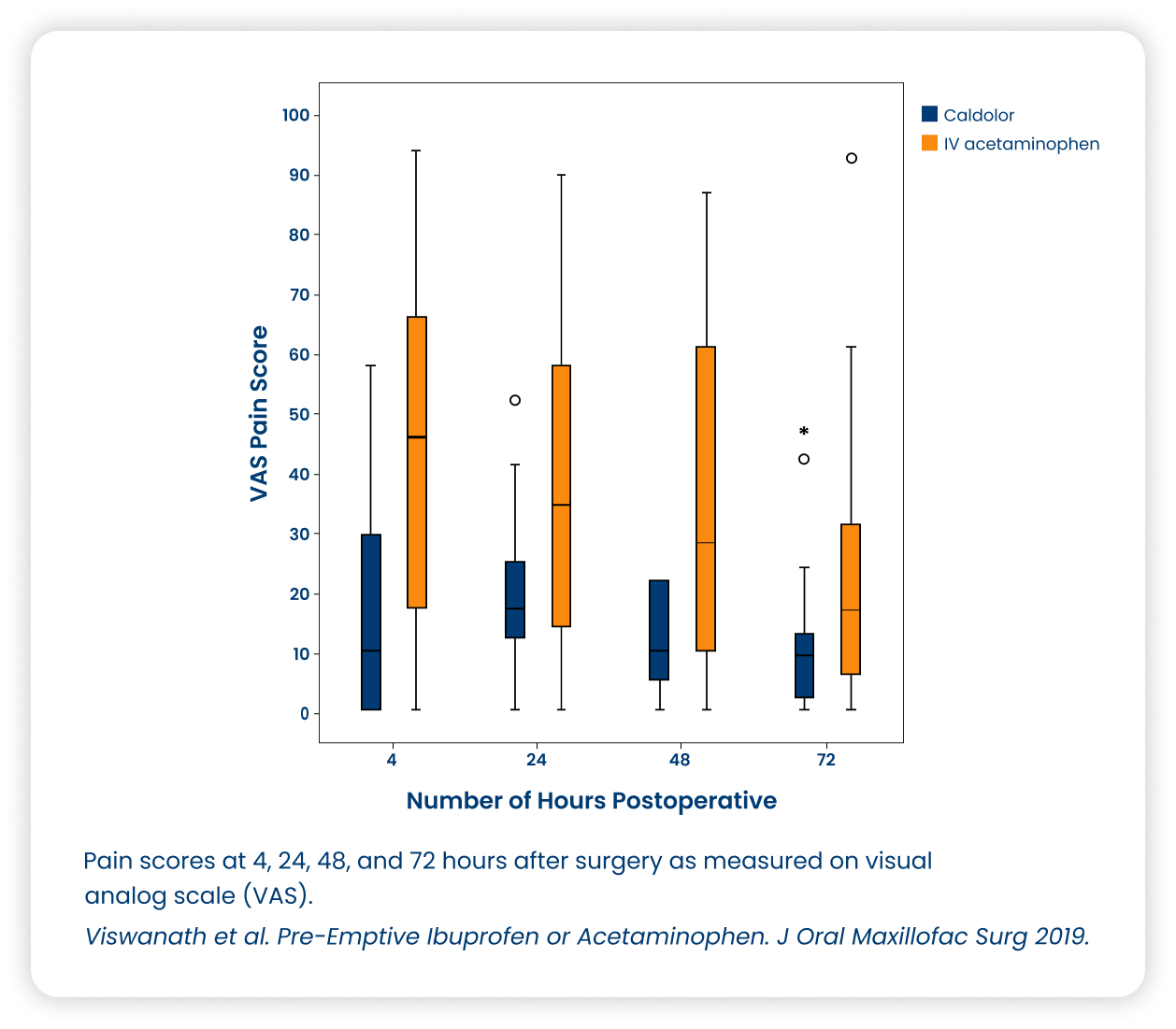
Postoperative pain scores in the Caldolor group were significantly lower than those in the IV acetaminophen group at 4 hours (p=0.004), 24 hours (p=0.019), and 48 hours (p=0.017).
After 72 hours, at the end of the acute inflammatory phase, reduced reported pain was an observed trend in the Caldolor group compared with the IV acetaminophen group.
Study description
Randomized, single-blinded conducted in patients undergoing surgical extraction of 2 or more impacted third molars under deep sedation.
Compared 2 interventions:
- 800 mg of Caldolor (Caldolor)
- 1,000 mg of IV acetaminophen (Ofirmev)
Primary outcome: postoperative pain measured on a visual analog scale at different time points.
Secondary outcome: amount of postoperative analgesic medication taken in both groups.
N = 58 (only 41 completed the study)
- Caldolor = 19
- IV acetaminophen = 22
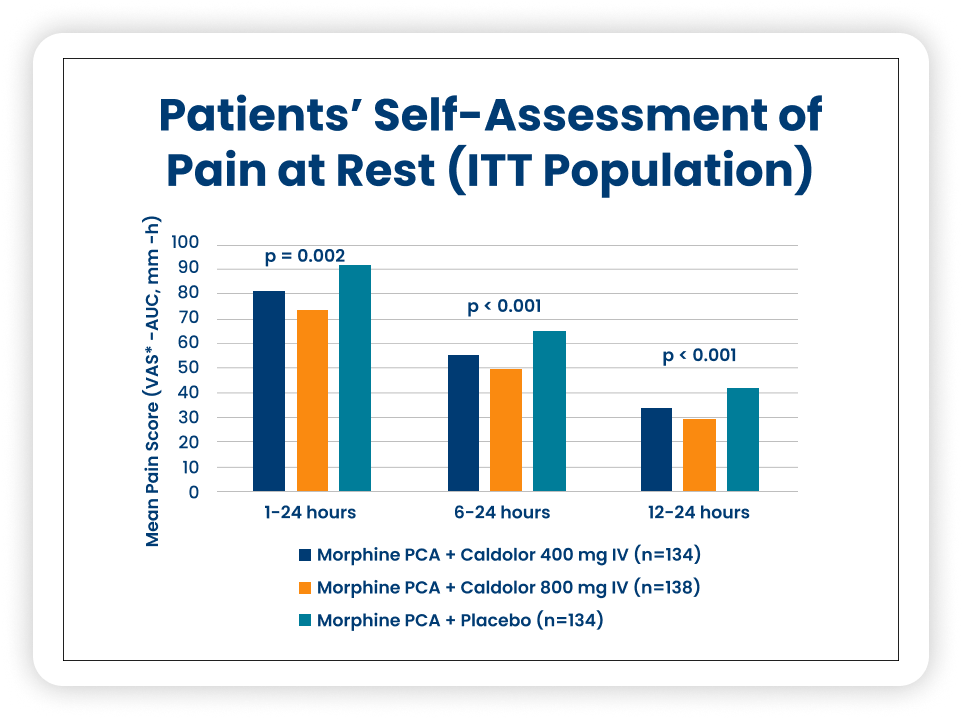
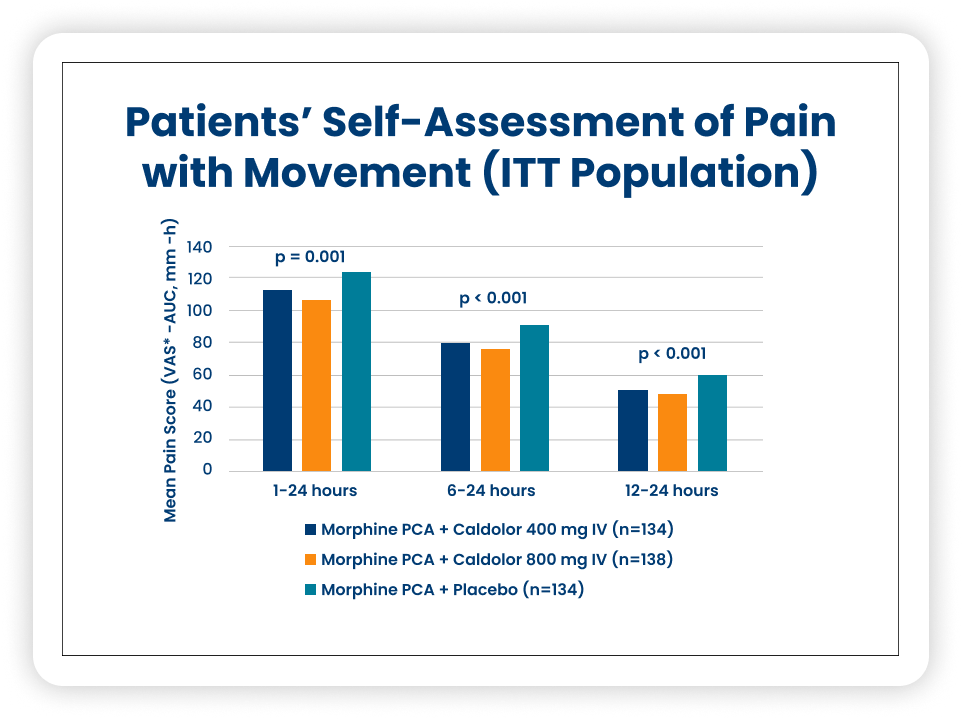
Elective Orthopedic or Abdominal Surgery5
Study description
Multi-center, randomized, double-blind, placebo-controlled trial in patients that underwent elective orthopedic or abdominal surgery.
- Randomized 1:1:1 Caldolor 400 mg, Caldolor 800 mg, placebo
- Dosed intra-op then every 6 hours x 8 doses (could continue up to 5 days (120 hours))
- Morphine PCA used for breakthrough pain
Primary Outcome: Morphine use in first 24 hours
Secondary Outcomes: Patient self-report scores at rest and with movement
N = 406
- Caldolor 400 mg: 134
- Caldolor 800 mg: 138
- Placebo: 134
Elective Abdominal Hysterectomy17
Study description
Multi-center, randomized, double-blind, placebo-controlled trial in female patients undergoing elective total abdominal hysterectomy and expected to be hospitalized post-op
- Randomized 1:1 Caldolor 800 mg or placebo
- Administered first dose at skin closure every 6 hours up to 5 days
- Morphine PCA used for breakthrough pain
Primary Outcome: Morphine requirement at 24 hours
Secondary endpoints: Self-reported pain intensity, time to first morphine dose, incidence of opioid-related ADRs, ambulation, time to liquid and solid intake, length of stay
N = 319
- Caldolor = 166
- Placebo = 153
Have Questions or Would like to Stay Informed About Caldolor?
We’re Here to Help!
